PennHIp Vs OFA
Below is a complete breakdown of both Hip Scoring Procedures. We currently use both methods to evaluate our breeding dogs.
The OFA Procedure
The OFA's Hip Radiograph Procedures
General Overview
Radiographs submitted to the OFA should follow the American Veterinary Medical Association recommendations for positioning. This view is accepted world wide for detection and assessment of hip joint irregularities and secondary arthritic hip joint changes. To obtain this view, the animal must be placed on its back in dorsal recumbency with the rear limbs extended and parallel to each other. The knees (stifles) are rotated internally and the pelvis is symmetric. Chemical restraint (anesthesia) to the point of relaxation is recommended. For elbows, the animal is placed on its side and the respective elbow is placed in an extreme flexed position.
The radiograph film must be permanently identified with the animal's registration number or name, date the radiograph was taken, and the veterinarian's name or hospital name. If this required information is illegible or missing, the OFA cannot accept the film for registration purposes. The owner should complete and sign the OFA application. It is important to record on the OFA application the animal's tattoo or microchip number in order for the OFA to submit results to the AKC. Sire and dam information should also be present.
Radiography of pregnant or estrus females should be avoided due to possible increased joint laxity (subluxation) from hormonal variations.OFA recommends radiographs be taken one month after weaning pups and one month before or after a heat cycle. Physical inactivity because of illness, weather, or the owner's management practices may also result in some degree of joint laxity. The OFA recommends evaluation when the dog is in good physical condition.
Chemical restraint (anesthesia) is not required by OFA but chemical restraint to the point of muscle relaxation is recommended. With chemical restraint optimum patient positioning is easier with minimal repeat radiographs (less radiation exposure) and a truer representation of the hip status is obtained.
For large and giant breed dogs, 14" x 17" film size is recommended. Small film sizes can be used for smaller breeds if the area between the sacrum and the stifles can be included.
If a copy is necessary ask your veterinarian to insert 2 films in the cassette prior to making the exposure. This will require about a 15% increase in the kVp to make an exact duplicate of the radiograph sent to OFA. Films may be returned if a $5.00 fee and request for return are both included at time of submission.
Good contrast is desirable (high mAs, low kVp). Grid techniques are recommended for all large dogs.
Radiation Safety
Proper collimation and protection of attendants is the responsibility of the veterinarian. Gonadal shielding is recommended for male dogs.
Mailing Recommendations
The radiograph, application and fees should be enclosed in a mailing envelope. These may be paper clipped together. Use the mail service of your choice. Obtain large envelopes from office supply store, veterinary hospital or other radiology department. The envelope should be sealed with tape. Light cardboard may be included to stiffen the package, but is not required. Avoid using boxes, tubes, padded envelopes, stapling check and application, bending/folding radiographs, or taping application or check to envelope.
OFA's Handling Procedures
When a radiograph arrives at the OFA, the information on the radiograph is checked against information on the application. The age of the dog is calculated, and the submitted fee is recorded. The board-certified veterinary radiologist on staff at the OFA screens the radiographs for diagnostic quality. If it is not suitable for diagnostic quality (poor positioning, too light, too dark or image blurring from motion), it is returned to the referring veterinarian with a written request that it be repeated. An application number is assigned.
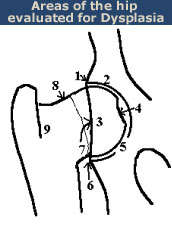
Radiographs of animals 24 months of age or older are independently evaluated by three randomly selected, board-certified veterinary radiologists from a pool of 20 to 25 consulting radiologists throughout the USA in private practice and academia. Each radiologist evaluates the animal's hip status considering the breed, sex, and age. There are approximately 9 different anatomic areas of the hip that are evaluated.
Craniolateral acetabular rim
Cranial acetabular margin
Femoral head (hip ball)
Fovea capitus (normal flattened area on hip ball)
Acetabular notch
Caudal acetabular rim
Dorsal acetabular margin
Junction of femoral head and neck
Trochanteric fossa
The radiologist is concerned with deviations in these structures from the breed normal. Congruency and confluence of the hip joint (degree of fit) are also considered which dictate the conformation differences within normal when there is an absence of radiographic findings consistent with HD. The radiologist will grade the hips with one of seven different physical (phenotypic) hip conformations: normal which includes excellent, good, or fair classifications, borderline or dysplastic which includes mild, moderate, or severe classifications.
Seven classifications are needed in order to establish heritability information (indexes) for a given breed of dog. Definition of these phenotypic classifications are as follows:
Excellent
Good
Fair
Borderline
Mild
Moderate
Severe
(See What Do Hip Grades Mean for more detail on the classifications)
The hip grades of excellent, good and fair are within normal limits and are given OFA numbers. This information is accepted by AKC on dogs with permanent identification and is in the public domain. Radiographs of borderline, mild, moderate and severely dysplastic hip grades are reviewed by the OFA radiologist and a radiographic report is generated documenting the abnormal radiographic findings. Unless the owner has chosen the open database, dysplastic hip grades are closed to public information.
Accuracy of Data
When results of 1.8 million radiographic evaluations by 45 radiologists were analyzed, it was found that all three radiologists agreed as to whether the dog should be classified as having a normal phenotype, borderline phenotype, or HD 94.9% of the time. In addition, 73.5% of the time, all three radiologists agreed on the same hip phenotype (excellent, fair, good, borderline, mild, moderate or severe). Twenty-one percent of the time, two radiologists agreed on the same hip grade and the third radiologist was within one hip grade of the other two. Two radiologists agreed on the same hip grade and the third radiologist was within two hip grades of the other two 5.4% of the time. This percentage of agreement is high considering the subjective nature of the evaluation.
Other Radiographic Findings
In addition to assessing the dog's hip conformation, the veterinary radiologist reports other radiographic findings that could have familial, inherited causes such as transitional vertebrae or spondylosis.
Transitional vertebrae are a congenital malformation of the spine that occur at the junctions of major divisions of the spine (usually between the thoracic and lumbar vertebral junction and the lumbar and sacral vertebral junction). Transitional vertebrae take on anatomic characteristics of both divisions of the spine it occurs between. The most common type of transitional vertebrae in dogs is in the lumbo-sacral area where the last lumbar vertebral body takes on anatomic characteristics of the sacrum. Transitional vertebrae are usually not associated with clinical signs and the dog can be used in a breeding program. The OFA recommends breeding the dog to another dog that does not have transitional vertebrae.
Spondylosis is another incidental radiographic finding where smooth new bone production is visualized between vertebral bodies at the intervertebral disc spaces. The new bone production can vary in extent from formation of small bone spurs to complete bridging of adjacent vertebral bodies. Spondylosis may occur secondary to spinal instability but often it is of unknown cause and clinically insignificant. A familial basis for its development has been reported. Like transitional vertebrae, dogs with spondylosis can be used in a breeding program.
THE PennHIP PROCEDURE
In 1937 veterinarian Gerry Schnelle wrote a paper entitled Bilateral Congenital Subluxation of the Coxofemoral Joints of a Dog. It was a landmark original description of what we today call Canine Hip Dysplasia. CHD for short, there are very few topics among dog owners, breeders, and veterinarians that can rival the spectrum of emotions evoked by this abnormality of the dog’s coxofemoral (hip) joint. The PennHIP procedure is a useful tool in determining the degree of hip joint laxity in dogs.
WHAT IS HIP DYSPLASIA
In short canine hip dysplasia (CHD) is a developmental abnormality of the hip joint. CHD is the most common orthopedic disease is dogs and is a polygenic (influenced by a number of genes) inherited trait. The radiographic changes observed with CHD include luxation or subluxation of the hip and osteoarthritis (degenerative joint disease). It is generally accepted and now scientifically proven that hip joint laxity (hip looseness) plays a major role in the development of osteoarthritis. Because osteoarthritis commonly causes pain and discomfort in the affected joints, the dog with CHD often has impaired mobility and a diminished quality of life. Therefore, any method that objectively measures hip joint laxity may be helpful in evaluating a dog’s risk for developing osteoarthritis and CHD. This information would assist the dog owner or breeder in deciding which animals not to breed as well as in selecting the best individual animals for breeding. Before we go further in this discussion of PennHIP, there are a few terms that are important to know. Take a look at the Definitions below and refer to them if you get confused.
CHD in many respects has been ignored by some, underestimated by a few and fervently analyzed by many. The evidence collected over the past 65 years since Dr. Schnelle first brought it to our attention has demonstrated that the presence of hip dysplasia in a dog has definite genetic determiners. More recently, data has been presented that shows the development of joint deterioration in a dog with CHD correlates well with the degree of joint laxity present in the dog. If hip laxity is present, other environmental factors, such as nutritional, can influence the degree of expression of abnormal signs associated with Canine Hip Dysplasia. The determination of the degree of CHD in a dog, the ultimate debilitative effects of any hip joint abnormality, the heritability factors for the potential offspring and the ethics of breeding a dog with CHD all factor into making this topic somewhat complicated… as the scientists say “It’s a multi-factorial subject”. Fortunately, however, the determination of degree of joint laxity using PennHIP Distraction Index is not subjective, but an accurate quantitative measurement.
TRADITIONAL EVALUATION
The ventrodorsal (front to back), hip-extended (legs pulled straight rearward) radiographic view as approved by the American Veterinary Medical Association in 1966 has been a standard for positioning of the dog on the x-ray table. The radiograph needs to be taken with the dog under sedation or anesthesia for proper and consistent positioning. If the positioning is not correct, the asymmetrical images of the hip joints will make accurate interpretation nearly impossible. This traditional and still widely accepted method of evaluating hip structure is used by many hip screening programs throughout the world, including Orthopedic Foundation for Animal (OFA), the Institute for Genetic Disease Control in Animals (GDC) and PennHIP. The OFA system and registry has been one strategy attempting to improve the knowledge base and selection process for breeders interested in eliminating CHD from a breed. Many breeders and veterinarians agree that the incidence of CHD has noticeably decreased over the years since it was first described, partly because awareness of CHD among pet owners and breeders has reached fairly high levels. For years the OFA protocol has been the most commonly utilized method of screening and certifying dogs as having normal or dysplastic hips. Unfortunately, subjective variables can enter into the OFA evaluation process. Although preliminary radiographs can be revealing, a potential drawback with the OFA protocol is the fact that for certification and definitive evaluation a dog must be 24 months of age or older at the time the hip radiographs are taken. Additionally, occasional criticism is heard that some veterinarians unknowingly affect the evaluation of the radiograph by their subjective positioning of the dog at the time the radiographs are taken; plus individual interpretation of what is visible on the radiograph is sometimes challenged. There exists the disappointing fact that outright fraud has occurred by unscrupulous individuals who misrepresent a radiograph as being of an animal other than the one actually radiographed.
PennHIP: (University of Pennsylvania Hip Improvement Program)
And that is precisely where the PennHIP topic becomes important. Commercially available since 1993, this procedure has been and was developed as an objective method of evaluating dogs’ hip structure. It evolved as a direct result of the subjectivity factors and age constraint (maturity) limitations inherent to evaluation and certification of dogs by the OFA and other screening programs. PennHIP research published in peer reviewed journals has shown that different breeds have different susceptibility to osteoarthritis. Therefore, in PennHIP evaluations each breed is compared to its own.
PennHIP incorporates an improved method for evaluating the integrity of the canine hip. It has great potential to lower the frequency of CHD when used as a breeding selection criterion. The technique assesses the quality of the canine hip and quantitatively measures canine hip joint laxity. Originally developed in 1983 by Gail Smith, VMD, PhD and his colleagues at the University of Pennsylvania, School of Veterinary Medicine, the procedure was conceived and developed as a new scientific method for an earlier and more accurate diagnosis of CHD. Years of research conducted in Smith’s laboratory proved the diagnostic method to be capable of estimating the risk (susceptibility) for CHD in dogs as young as sixteen weeks of age.
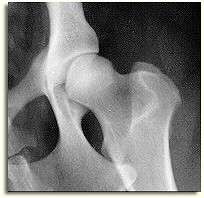
It is especially important to perform a Distraction Index (DI) on dogs that have normal appearing hips on the ventrodorsal extended view, such as appears to be the case in the image on the right. Dogs that are diagnosed as having excellent hips on the traditional VD view can actually have a huge amount of laxity. PennHIP's recommendation is to limit breeding to those dogs that have normal appearing hips on the VD hip extended view and that also have a DI at the breed's mean laxity or tighter.
The PennHIP method is a novel way to assess, measure and interpret hip joint laxity and hip conformation. Three separate radiographs are taken of a sedated or anesthetized dog…
* the distraction view
* the compression view
* the standard ventrodorsal, hip-extended view.
The distraction view and compression view are used to obtain accurate and precise numerical measurements of joint laxity and conformation. The hip-extended view is used to diagnose osteoarthritis using criteria similar to the OFA and other hip screening organizations. Precise positioning of the dog by trained certified PennHIP members is imperative and any radiographs that do not conform to prescribed positioning are rejected and must be repeated.
Interestingly, a dog's hip laxity at 16 weeks of age will be much the same at one year, two years and older. For most breeds, the PennHIP evaluation can be done as early as four months of age. Recommendations based upon peer reviewed and published research, though, state that the reliability of the PennHIP method slightly improves with age, with one year being marginally superior to six months, which in turn is marginally better than four months. The Distraction Index (DI), obtained via the distraction view radiograph, is not subjective. It is an accurate numerical measurement that has been shown to be reliable.
DISTRACTION INDEX
Also called the DI, the Distraction Index is obtained with the aid of a fulcrum so that a radiograph can be taken with the head of the femur as far out of the hip socket as possible. This distance is then measured. Hips with DIs on the distraction view that are close to 0 are considered to be tight, while DIs close to 1 are considered to be very loose. The DI is an indication of the "percent out of joint" that the femoral head is displaced from the acetabulum (socket). For example, DI=0.58 means the femoral head comes out of the joint by 58%, DI=0.75, 75% out of joint and so on.The Distraction Index of PennHIP is not subjective, but an accurate quantitative measurement that has been shown to be repeatable and reliable. A dog with a DI approaching 1 has a very high degree of predictability for developing Canine Hip Dysplasia and subsequent osteoarthritis... and should not be considered for breeding purposes.
WHO DOES PennHIP PROCEDURES
Only certified individuals who have undergone special training and have successfully demonstrated their expertise in the technique are permitted to perform PennHIP procedures. Since both PennHIP and OFA use the ventrodorsal, hip-extended view, your PennHIP certified veterinarian can make a copy of the hip-extended radiograph for submission to the OFA at the time your dog has the PennHIP procedure. You do not have to abandon OFA opinion nor schedule a separate appointment for an additional radiograph.
As of November 2001, there were 1,076 certified PennHIP members. 977 members are in the United States and Canada and 99 in 19 other countries. Darryl N. Biery, DVM, Professor of Radiology and a Board Certified Veterinary Radiologist at the School of Veterinary Medicine, University of Pennsylvania states, “All PennHIP certified veterinarians have passed a certification process that includes course work and quality control supervision.”
With the devastating effects of CHD, the PennHIP procedure is a welcomed addition to the opportunities dog breeders have in selecting only the best individuals for carrying on the ideal traits of each breed. That selection flexibility is enhanced by the opportunity to go beyond the qualitative description of calling a hip joint “normal” by actually applying a numerical value to “normal” and abnormal joints. That numerical value is called the Distraction Index (DI). With PennHIP the breeder can make a more appropriate choice among breeding individuals with “normal hips” by referring to the Distraction Index and selecting the best individuals in the “normal” group… the ones with the tightest hips.
The PennHIP Laboratory publishes its findings in scientific journals. Published information is disseminated to all PennHIP members; it is also shared with interested breed clubs and routinely appears in publications within the dog fancy. Will the PennHIP protocol replace the traditional OFA protocol? Only time will tell. But this newer method of evaluating dogs’ hip joints will be one more tool to improve future generations of dogs. So for all of us who love and respect canines, the PennHIP procedure should be a welcomed addition to our diagnostic and predictive treasure chest.
ADVANTAGES OF PennHIP
There are a number of advantages associated with doing the PennHIP procedure rather than the traditional method of radiography:
The PennHIP Procedure is...
* A scientifically validated method.
* Performed on dogs as young as 16 weeks of age.
* 2.5 –11 times more hip laxity is measured compared to the conventional ventrodorsal, hip-extended radiographic evaluation method. This objective measurement of hip joint laxity is critical since the amount of laxity detected has a direct relationship to the likelihood that a dog will develop arthritis (the looser the hip the greater the risk).
* PennHIP radiographic score has a higher heritability coefficient, and therefore has a greater potential to improve hips through selective breeding than the ventrodorsal, hip-extended view alone.
* Requires mandatory submission of hip films to minimize bias in database. (Even hips showing obvious dysplasia are sent in and added to the database.)
PennHIP OR OFA?
What procedure should a dog owner select when attempting to gain valid information about a dog’s hip status? I posed this question: “What is the major difference between having a dog evaluated by the OFA as opposed to having a PennHIP evaluation done?” In response Dr. Smith states, “The PennHIP radiographic evaluation has been shown scientifically to give a truer estimate of hip quality; it is more accurate, more reliable and as mentioned it can be performed as early as 16 weeks of age. The major advantage of the PennHIP method is its unique ability to identify true-normal dogs, dogs not susceptible to hip dysplasia.”
Small animal practitioner Mara DiGrazia, DVM, of New Hyde Park, N.Y., although not PennHIP certified, states her approach to the question of which procedure to use: “If a client has a young puppy that they are considering to use for breeding I would recommend the PennHIP radiographs rather than waiting for an OFA. This is because PennHIP can predict as early as 4 months of age what degree of hip dysplasia the dog may develop. Early OFA radiographs may not reveal the same degree of laxity in the joint. Early identification of hip deformity can make a world of difference to the dog’s future life. The PennHIP procedure can bring about a timely spay or neuter if the dog has been found to be unworthy of breeding due to poor hip conformation. The dog’s lifestyle can then conform to its needs as a pet rather than as a working or breeding dog.“
Definitionof terms:
Articular Cartilage, nourished by synovial fluid, is the cartilaginous surface of the end of a bone, which contributes to the function of a joint.
Osteoarthritis, Degenerative Joint Disease (DJD) is marked by degeneration or breakdown of the articular cartilage, hypertrophy of bone at the margins of the joint, and changes in the synovial membrane and joint capsule, and is accompanied by pain and stiffness.
Joint Laxity refers to the amount of looseness in a joint. Generally the more laxity the greater the potential for DJD from the trauma associated with loosely fitting joint members.
Luxation means dislocation. A luxated hip is one that has extreme laxity such that it displays dislocation of the two bones of the joint. The x-ray image at the top right of this page demonstrates a fully luxated hip on the right side of the image.
Subluxation means a partial dislocation of two joint members. The x-ray image at the top right of this page demonstrates a subluxated hip on the left side of the image.
The ventrodorsal, hip-extended radiographic view: This refers to the standard positioning of the dog on its back on the X-ray table. The radiograph is made with the beam projection from the front to the back of the dog while the rear legs are pulled symmetrically rearward. To be done properly, the view is generally done under sedation or anesthesia.
OFA Update: The Issue of Joint Laxity and Stress Radiography By G.G. Keller, D.V.M., MS, Diplomate of A.V.C.R., Executive Director Orthopedic Foundation for Animals, Inc. and E.A. Corley, D.V.M., Ph.D., Diplomate of A.V.C.R.
OFA does not normally respond to the various opinions expressed by individuals on Internet web sites and/or chat lines. Instead OFA maintains a web site (http://www.offa.org) to provide information that may be of value to breeders and veterinarians. However, a response to the opinions expressed by many people is prompted, as the opinions appear to have deteriorated to the point of becoming non-productive. OFA stated its position on any testing method, including PennHIP, that involved stress radiography to the breed clubs in 1994. This posting is a review of that position.
Contrary to some Internet postings, OFA, a not-for-profit organization, does support and encourage research on joint laxity and its meaning. The fact that joint laxity plays a role, but is not the only factor to be considered in development of hip dysplasia and its secondary changes of degenerative joint disease, has been recognized for over 30 years. This fact is not in dispute. T he issue has been, and remains to be, the relationship of laxity that is demonstrated by forcing the heads of the femurs away from the acetabula by palpation or a fulcrum/stress device (i.e., a distraction device) to abnormal laxity (functional laxity that occurs in hip dysplasia.) Since 1972, when an independent panel of scientists classified the techniques for demonstration of joint laxity by use of an externally applied force as experimental, OFA has financially supported three research projects, recommended by external review, to answer the basic question. Dr. Belkoff, et.al. (VCOT 1: 31-36 1989) developed a device that measured the amount of force applied to the hips and noted that some dogs that demonstrated abnormal amounts of laxity were free of hip dysplasia at necropsy. These authors questioned the meaning of joint laxity as demonstrated by force. The other two projects supported by OFA are ongoing.
PennHIP is another technique for demonstration of forced (passive) laxity that is also attempting to answer the basic question of the relationship of passive laxity to functional laxity. OFA encourages their research efforts; however, OFA takes exception to the marketing techniques and claims used to promote the PennHIP testing method for clinical use, as the use of this method appears to be premature. In other words, commercialization (marketing) of the method has outreached the science.
OFA feels that general use of PennHIP as a mass screening test method for hip dysplasia is prematur e because:
- The primary basis for marketing PennHIP was reported by Dr. Smith, et.al. (Am J Vet Res, July 1993) using a modification of a previously described positioning, stress/fulcrum technique. The study was a survey type involving 142 dogs (105 of which were German Shepherd Dogs). The results of the study were questioned by Dr. Susan Shott of the Biostatistical Unit, Rusk Cancer Institute (Am J Vet Res, December 1993) who challenged the analysis of the data and stated: "The data does not support the author’s conclusion that the DI was the most important and reliable phenotypic factor for determining susceptibility of hips to degenerative joint disease ... and that this determination could be made with an acceptable degree of accuracy as early as 4 months of age."
- Dr. Lust, et.al. (Dr. Smith was a coauthor) in a report involving 42 Labrador Retrievers (Am J Vet Res, December 1993) concluded that a DI of <0.4 at 4 months of age correctly predicted normal hips in 88% of the cases and a DI of >0.4 correctly predicted hip dysplasia in 57% of the cases. The authors further concluded that: "Distraction indices between 0.4 and 0.7 and at either 4 or 8 months of age were not associated strongly enough with evidence of disease to be clinically reliable in predicting, on an individual basis, the outcome for dysplastic hip conformation when the dogs were older."
- No breeding data based on PennHIP h as been reported. Dr. E.A. Leighton (JAVMA, May 13, 1997) reported on genetic progress in improving the hip quality in German Shepherd Dogs and Labrador Retrievers in the Seeing Eye closed colony of dogs. In less than 5 generations the percentage of hip dysplasia was decreased from 55 to 24% in the German Shepherd Dogs and from 30 to 10% in the Labrador Retrievers using the hip extended position and a modified OFA evaluation procedure. PennHIP DI measurements were also made but the mean DI across generations did not change. It should be pointed out that DI was considered experimental and breeding selection criteria did not include the DI. It will be interesting to see the results when DI is included as a selection criterion.
With the above reservations, plus experience with the issue of joint laxity, OFA would be remiss in its responsibility to either endorse or reject the PennHIP testing method. In other words, the jury is still out! This leaves the breeder in a dilemma as to which testing method to use, OFA or PennHIP or both, as they are entirely different test methods for the same disease.
There is a great economic advantage to breeders for determination of the hip status at a young age and to assess the risk for development of hip dysplasia at a later age. OFA reported (Vet Clinics of No Am, May 1992) on a study of 3,369 dogs from 25 breeds. Reliability of the preliminary evaluations ranged from 71.4% in the Chesapeake Bay Retriever to 100% in the Welsh=2 0Springer Spaniel. The preliminary evaluation appeared to be breed dependent and dependent on the evaluator’s experience with the skeletal development of that breed at the age of evaluation.
When faced with the problem of comparing entirely different test methods for determining dysplasia, scientists evaluate the results of reported values for false negative (probability of diagnosing a dysplastic dog as normal), false positive (probability of diagnosing a normal dog as dysplastic), specificity (probability of a normal dog receiving a normal evaluation), and sensitivity (probability of a dysplastic dog receiving a dysplastic evaluation). These values for OFA preliminary evaluations by age and hip ratings, in a different population of dogs than previously reported (Vet Clinics of No Am., May 1992) have been reported (JAVMA, November 1, 1997). The false negative and false positive values for PennHIP were reported by Dr. Smith et.al. (Am J Vet Res, July 1993). No report of selectivity or sensitivity values for PennHIP were given. There were 2,332 dogs in this OFA study and 142 dogs in the PennHIP study. The limited number of dogs resulted in a larger confidence interval for the PennHIP values. Confidence intervals (CI) are determined so that one can be 95% confident that the true value lies within the calculated range. The false negative values for OFA evaluations were 8.9% (CI=5.9 to 12.9%) at 3-6 months, 6.0% (CI=4.4 to 8.0%) at 7-12 months and 3.8% (CI=2.6 to 5.4%) at 13-18 months of age. The false ne gative values for PennHIP evaluations were 12% (CI=1.5 to 38.3%) at 4 months and 0% (CI=0.0 to 15.4%) at 12 months of age. It appears that the probability of retaining a dysplastic dog in the breeding pool is the same for either test method.
However, the false positive values for PennHIP were significantly greater (48% at 4 months, 57% at 6 months and 38% at 12 months) than those for OFA evaluations 17.6% at 3-6 months (CI 10.8 to 26.4%), 10.0% at 7-12 months (CI 5.7 to 15.9%) and 8.5% at 13-18 months (CI 4.8 to 13.6%). It appears that the probability for removing a normal dog from the breeding pool is less with the OFA evaluations.
Dr. Adams, et.al. (JAAHA, 1998, 34: 339-47) reported (using palpation, OFA method, PennHIP, and Norberg angle measurements) on results of a study of hip laxity, in 32 dogs from 4 breeds (12 Greyhounds, 4 Labrador Retrievers, 12 Irish Setters, and 4 hound-mix) at 6-10 weeks and 16 to 18 weeks that were compared to detection of degenerative joint disease at 52 weeks of age. Five hips with evidence of subluxation but no evidence of degenerative joint disease on the OFA type evaluation of the hip extended view were eliminated from analysis. The authors concluded that DI and Norberg Angle measurements at 6-10 and 16-18 weeks were the most reliable predictors of hip dysplasia, at 52 weeks of age, with DI being more reliable than Norberg. The OFA and palpation methods at 6-10 or 16-18 weeks were not reliable predictors. This is not s urprising as reliability of OFA preliminary evaluations has been shown to increase with age of evaluation. The OFA report (JAVMA, Nov. 1997) included 380 dogs evaluated at 3 to 6 months of age. The reliability was 89.6% (CI=85.4 to 92.9%) for normal evaluations and 80.4% (CI=71.4 to 87.6%) for dysplastic evaluations. The mean age was 4.8 months (19.2 weeks) and the median age was 5 months (20 weeks) which means that over half of the dogs in the OFA study were older than in the study reported by Dr. Adams.
OFA data and PennHIP data are not representative of the general population of dogs because the programs are voluntary, most dogs are in pet homes and are not radiographed, and not all radiographs of dogs radiographed are submitted for evaluation by either program. For example; if an attending veterinarian determines a dog to be dysplastic, by either method, the radiograph(s) may not be submitted to save the owner money. PennHIP collaborators may take the hip extended view first and if the radiograph shows evidence of dysplasia the DI views may not be taken or the owner may not allow submission of an obviously large DI measurement.
Breeders are aware of the economic value of early screening of dogs for determination of the hip status. They should also be aware that both OFA and PennHIP use the radiographic evaluation of the same hip extended projection as the standard for comparing with the results of the early evaluations. The OFA standard represents the consensus of203 independent evaluations at >24 months of age by board certified veterinary radiologists. It is not clear who evaluates a radiograph submitted for PennHIP determination, but the original study reported the standard to be Dr. Smith’s evaluation. This evaluation at >24 months of age has approximately 5% false negative finding as reported by Dr. Jessen (Proceedings of a 1972 symposium on hip dysplasia) and by an internal OFA study of dogs evaluated at 24 months that were re-evaluated at an older age. This is why OFA requires the 24 month certification age. Voluntary submissions to PennHIP will provide information on the range, mean and median of the DI measurements for the various breeds. The meaning of the measurements remains unclear and will require repeat studies, on the same dogs, at >24 months of age.
Breeders must be aware of the cost, strengths, and weaknesses of the test methods available for evaluation of the hip status before making the choice of a specific testing method. Once the choice is made, it must be followed for generations before progress in improving the hip status can be evaluated. OFA data has demonstrated marked improvement of the hip status in the Portuguese Water Dog (AKC Gazette, Nov 1991) and the Chinese Shar Pei (Barker, Mar/Apr 1995). OFA data on all breeds was independently evaluated and reported by Dr. Kaneene (JAVMA, Dec 1997) an epidemiologists from the Population Medicine Center at Michigan State University. The study compared OFA evaluatio ns on dogs born between 1972 and 1980 with dogs born between 1989 and 1992. The population consisted of 270,978 dogs. The authors, having acknowledged the fact that submissions are voluntary and that there is bias due to prior screening, concluded:
We do not believe that this is the most likely explanation, because the increase in the percentage of dogs classified as having excellent hip joint phenotype (+36% [7.82 vs 10.64%]) was substantially larger than the decrease in the percentage of dogs classified as having canine hip dysplasia (-21.% [17.39 vs 13.82%]). If better screening of radiographs prior to submission to the OFA was the cause of the increase in percentage of dogs classified as having an excellent hip joint phenotype, then because it is easier to differentiate dysplastic hips from hips with normal phenotypes than it is to differentiate hips with excellent, good and fair phenotypes, we would have expected that the decrease in percentage of dogs classified as having canine hip dysplasia would have been larger than the increase in percentage of dogs classified as having an excellent hip joint phenotype.
Unfortunately, PennHIP has not been available long enough to accumulate the data necessary to evaluate the effect of this test method over time.
G.G. Keller, D.V.M., MS, Diplomate of A.V.C.R., is the Executive Director of Orthopedic Foundation for Animals, Inc. Dr. Keller received his Doctorate in Veterinary Medicine in 1973 an d was in a small animal private practice until 1987 at which time he accepted the Associate Director position for the Orthopedic Foundation for Animals. He received the Masters degree in Veterinary Medicine and Surgery in 1990 and Diplomate status in the American College of Veterinary Radiology in 1994. He assumed the role of Executive Director for the Orthopedic Foundation for Animals in January, 1997.
To contact the OFA:
2300 E. Nifong Blvd.
Columbia, MO 65201
Tel: 573-442-0418
Fax: 573-875-5073
Email: ofa@offa.org
Web site: http://www.offa.org
Original article text copyright 1998 by Orthopedic Foundation for Animals. This article may be reprinted in paper form for educational purposes only, with the OFA copyright notice intact.
This article is a special feature of and was first published on Workingdogs.com. If you wish to link to this article from your web site, please contact the Working Dogs Cyberzine Publisher for linking permissions. Permission is not granted to copy the code or design from this page to any other. Copyright 1998-2005 Working Dogs; all rights reserv
Penn Hip vs OFA
by Gordon Theilen, DVM
There has been good discussion about value of Penn Hip and that of OFA. I would like to emphasize a few important aspects for all to remember in their breeding programs. Some of the following has already been said and given here as important points to remember.
1) Penn Hip measures hip laxity not dysplasia which also is called arthritis. Young dogs are radiographed under sedation and pressure is applied to attempt to move the head of the femur out of the pelvic joint socket that is held in place by the central round ligament. Then radiographs taken are sent to University of Pennsylvania, College of Veterinary Medicine and radiologists there rate the hips ( Penn Hips) using a distraction index formula and determine the quotient up to 1. The ratings very for each breed and usually a 0.4 or higher rating is undesirable. Dogs with a high fraction will be AFFECTED DOGS and show lameness. I have forgotten the desirable fraction for the Brittany, but it is around 0.4 or lower. The Penn Hip procedure does not harm the pup. If there is a hip joint laxity of 0.4 or more it was genetic and not caused by the procedure. Gene markers have been found for hip laxity in some breeds and the left hip joint has a higher percentage of frequency than the right hip. Laxity is under genetic control and not the same as canine hip dsyplasia ( CHD). Some dogs with CHD occur concurrently with those that have hip laxity, but the two are genetically separate entities.
2) Canine hip dsyplasia are bone changes that start from embryonic life ( under genetic control) and may not be detected for years, but up to 95% are detected by 2 years of age, the time that Orthopedic Foundation for Animals ( OFA ) certifies hips and elbows with radiographs. Most dysplastic hips can be detected by 6 to 8 months of age, upwards of 85 to 90% occur by that age. Thus, it is recommended to have hip preliminaries done early about 6 months of age and before 2 years of age. A dysplastic pup at 6 months will never have good hips at a later age. Another value of OFA is knowing families being free or at very low frequency for CHD for up to 3 generations including not only sire/dam, grandsire/grandam, and great grandsire/great granddam but also related relatives, sibs, cousins, aunts, uncles etc. This helps establish frequency of CARRIER DOGS. It is generally obvious which dogs are dysplastic, however, CARRIER DOGS are normal and may be categorized as excellent, good or fair. Excellent does not necessarily mean there is less chance for being a CARRIER, it only means that dog has excellent hips, not genetically free of CARRYING CHD.
3) Dogs that are Pen Hip with a low distraction index and OFA normal can still be CARRIERS. Dogs with normal hips can still be CARRIER DOGS. The condition that so many neglect to know about or recognize. CARRIERS are the key to riding unwanted genes from the population. The only real way to effectively do this is by open registry and or OPENNESS by all breeders. Brittany owners and breeders should consider as a breed club becoming members of Canine Health Information Center ( CHIC). The mission: to provide a source of health information for owners, breeders, and scientists, which will assist in breeding healthy dogs. CHIC is an organization that works together with OFA and AKC Canine Health Foundation. As of September 2004 over 30 parent breed clubs had become members of CHIC. You can find out more about CHIC by seeing or .
4) To find CARRIER DOGS one can do this by carefully keeping records and being aware of the health and or unhealthy condition of offspring from dogs you wish to purchase a pup or breed for a litter. Fortunately we now have at our disposal modern technology as well to combine with the art of breeding.
5) DNA profile of your dog and family of dogs can help find CARRIER DOGS. UCD, School of Veterinary Medicine, Division of Canine Genetics will send DNA swabs free of charge to any Brittany owner desiring to have their dogs entered into the Brittany DNA Bank. It will take thousands of samples to have an effective DNA Bank. Many persons across the Nation are now collecting and aiding Scientists at UCD develop this Bank. Laboratory personal are desirous of ABC becoming members of CHIC and together we hopefully will find CARRIER DOGS for not only hips and elbows but for a myriad of other health and trait problems. It also will be a repository for documenting and maintaining wanted health and traits. Contact kathryn Robertson < krrobertson@ucdavis.edu> for swabs. For serious questions on genetics contact Mark Neff PhD < mwneff@ucdavis.edu>, in charge of Brittany DNA Studies or for lesser technical questions contact me. Please let me know as chairman of the Health Aspects and Genetic Defects Committee of ABC whether we should pursue membership as a parent club in CHIC.
6) CARRIER DOGS can not easily be found using DNA unless there are thousands of samples at the scientist disposal.
7) MAINTAINING GENETICALLY STRONG DOGS can not easily be documented without thousands of DNA samples.
We as a breed are extremely fortunate to have the Brittany DNA Bank established at UCD, few breeds have such an opportunity. This was all made possible by the Marvin D. Nelson Jr. Memorial Fund established in 2004 by ABC. Of the $30,000 so far donated, none of the monies have been spent, all have been banked until the Fund substantially grows hopefully to 1/2 to one million dollars. Thus, donations are always needed, so we as Brittany owners can say we have contributed directly to finding genetic make up for maintaining genetically strong breeding stock or for finding CARRIER DOGS for unwanted health problem or traits and develop breeding strategies to handle the unwanted. This type of research is very expensive and we must develop more ways to help pay for needed research. For donations see Trust this helps all appreciate what CARRIER DOGS are all about and why they are the nemesis in all good breeding programs to maintain and better the breed.